


 Sign Out
Sign Out

PHARMACOLOGY: Pharmacodynamics: The precise mechanism of action of gabapentin is not known.
Gabapentin is structurally related to the neurotransmitter GABA (gamma-aminobutyric acid) but its mechanism of action is different from that of several other active substances that interact with GABA synapses including valproate, barbiturates, benzodiazepines, GABA transaminase inhibitors, GABA uptake inhibitors, GABA agonists, and GABA prodrugs. In vitro studies with radiolabeled gabapentin have characterized a novel peptide binding site in rat brain tissues including neocortex and hippocampus that may relate to anticonvulsant and analgesic activity of gabapentin and its structural derivatives. The binding site for gabapentin has been identified as the alpha2-delta subunit of voltage-gated calcium channels.
Gabapentin at relevant clinical concentrations does not bind to other common drug or neurotransmitter receptors of the brain including GABAA, GABAB, benzodiazepine, glutamate, glycine or N-methyl-d-aspartate receptors.
Gabapentin does not interact with sodium channels in vitro and so differs from phenytoin and carbamazepine. Gabapentin partially reduces responses to the glutamate agonist N-methyl-D-aspartate (NMD) in some test systems in vitro, but only at concentrations greater than 100 μM, which are not achieved in vivo. Gabapentin slightly reduces the release of monoamine neurotransmitters in vitro. Gabapentin administration to rats increases GABA turnover in several brain regions in a manner similar to valproate sodium, although in different regions of brain. The relevance of these various actions of gabapentin to the anticonvulsant effects remains to be established. In animals, gabapentin readily enters the brain and prevents seizures from maximal electroshock, from chemical convulsants including inhibitors of GABA synthesis, and in genetic models of seizures.
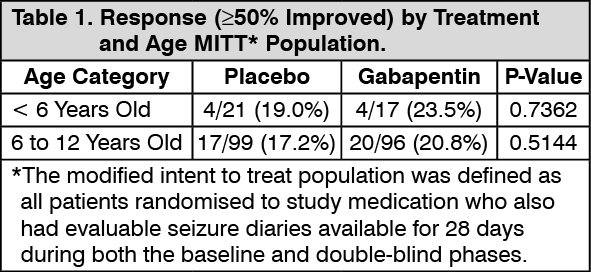
A clinical trial of adjunctive treatment of partial seizures in paediatric subjects, ranging in age from 3 to 12 years, showed a numerical but not statistically significant difference in the 50% responder rate in favour of the gabapentin group compared to placebo. Additional post-hoc analyses of the responder rates by age did not reveal a statistically significant effect of age, either as a continuous or dichotomous variable (age groups 3-5 and 6-12 years). The data from this additional post-hoc analysis are summarised in the table as follows: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: Following oral administration, peak plasma gabapentin concentrations are observed within 2 to 3 hours. Gabapentin bioavailability (fraction of dose absorbed) tends to decrease with increasing dose. Absolute bioavailability of a 300 mg capsule is approximately 60%. Food, including a high-fat diet, has no clinically significant effect on gabapentin pharmacokinetics.
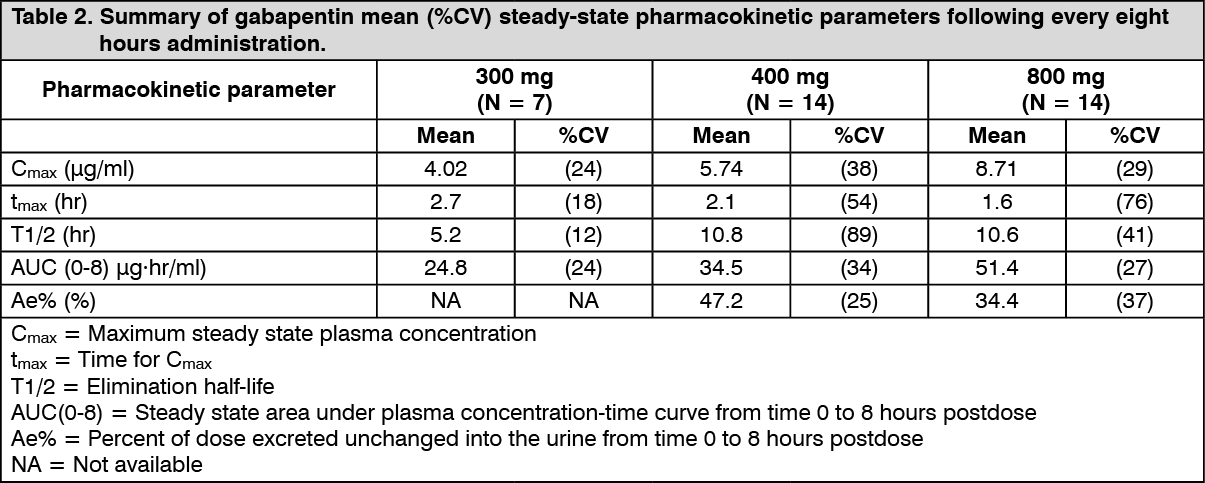
Gabapentin-pharmacokinetics are not affected by repeated administration. Although plasma gabapentin concentrations were generally between 2 μg/ml and 20 μg/ml in clinical studies, such concentrations were not predictive of safety or efficacy. Pharmacokinetic parameters are given in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDistribution: Gabapentin is not bound to plasma proteins and has a volume of distribution equal to 57.7 litres. In patients with epilepsy, gabapentin concentrations in cerebrospinal fluid (CSF) are approximately 20% of corresponding steady-state trough plasma concentrations. Gabapentin is present in the breast milk of breast-feeding women.
Biotransformation: There is no evidence of gabapentin metabolism in humans. Gabapentin does not induce hepatic mixed function oxidase enzymes responsible for drug metabolism.
Elimination: Gabapentin is eliminated unchanged solely by renal excretion. The elimination half-life of gabapentin is independent of dose and averages 5 to 7 hours.
In elderly patients, and in patients with impaired renal function, gabapentin plasma clearance is reduced. Gabapentin elimination-rate constant, plasma clearance, and renal clearance are directly proportional to creatinine clearance.
Gabapentin is removed from plasma by haemodialysis. Dosage adjustment in patients with compromised renal function or undergoing haemodialysis is recommended (see Dosage & Administration).
Gabapentin pharmacokinetics in children were determined in 50 healthy subjects between the ages of 1 month and 12 years. In general, plasma gabapentin concentrations in children >5 years of age are similar to those in adults when dosed on a mg/kg basis.
In a pharmacokinetic study in 24 healthy paediatric subjects aged between 1 month and 48 months, an approximately 30% lower exposure (AUC), lower Cmax and higher clearance per body weight have been observed in comparison to available reported data in children older than 5 years.
Linearity/Non-linearity: Gabapentin bioavailability (fraction of dose absorbed) decreases with increasing dose which imparts non-linearity to pharmacokinetic parameters which include the bioavailability parameter (F) e.g. Ae%, CUF, Vd/F.
Elimination pharmacokinetics (pharmacokinetic parameters which do not include F such as CLr and T½), are best described by linear pharmacokinetics. Steady state plasma gabapentin concentrations are predictable from single-dose data.
Toxicology: Preclinical safety data: Carcinogenesis: Gabapentin was given in the diet to mice at 200, 600, and 2000 mg/kg/day and to rats at 250, 1000, and 2000 mg/kg/day for two years. A statistically significant increase in the incidence of pancreatic acinar cell tumors was found only in male rats at the highest dose. Peak plasma drug concentrations in rats at 2000 mg/kg/day are 10 times higher than plasma concentrations in humans given 3600 mg/day. The pancreatic acinar cell tumors in male rats are low-grade malignancies, did not affect survival, did not metastasize or invade surrounding tissue, and were similar to those seen in concurrent controls. The relevance of these pancreatic acinar cell tumors in male rats to carcinogenic risk in humans is unclear.
Mutagenesis: Gabapentin demonstrated no genotoxic potential. It was not mutagenic in vitro in standard assays using bacterial or mammalian cells. Gabapentin did not induce structural chromosome aberrations in mammalian cells in vitro or in vivo, and did not induce micronucleus formation in the bone marrow of hamsters.
Impairment of Fertility: No adverse effects on fertility or reproduction were observed in rats at doses up to 2000 mg/kg (approximately five times the maximum daily human dose on a mg/m2 of body surface area basis).
Teratogenesis: Gabapentin did not increase the incidence of malformations, compared to controls, in the offspring of mice, rats, or rabbits at doses up to 50, 30 and 25 times respectively, the daily human dose of 3600 mg, (four, five or eight times, respectively, the human daily dose on a mg/m2 basis).
Gabapentin induced delayed ossification in the skull, vertebrae, forelimbs, and hindlimbs in rodents, indicative of fetal growth retardation. These effects occurred when pregnant mice received oral doses of 1000 or 3000 mg/kg/day during organogenesis and in rats given 500, 1000, or 2000 mg/kg prior to and during mating and throughout gestation. These doses are approximately 1 to 5 times the human dose of 3600 mg on a mg/m2 basis.
No effects were observed in pregnant mice given 500 mg/kg/day (approximately ½ of the daily human dose on a mg/m2 basis).
An increased incidence of hydroureter and/or hydronephrosis was observed in rats given 2000 mg/kg/day in a fertility and general reproduction study, 1500 mg/kg/day in a teratology study, and 500, 1000, and 2000 mg/kg/day in a perinatal and postnatal study. The significance of these findings is unknown, but they have been associated with delayed development. These doses are also approximately 1 to 5 times the human dose of 3600 mg on a mg/m2 basis. In a teratology study in rabbits, an increased incidence of post-implantation fetal loss, occurred in doses given 60, 300, and 1500 mg/kg/day during organogenesis. These doses are approximately ¼ to 8 times the daily human dose of 3600 mg on a mg/m2 basis.